

Shanti Mathias visits a volunteer-run milk bank, where donated breast milk is processed and distributed to newborns in need.
The milk is in bottles with light blue tops, neatly labelled, the three fridges humming steadily to keep the liquid cool. But a closer look at the milk shows not the pale white of Anchor or Meadow Fresh but a light yellow colour: this is colostrum-rich human milk, stored at a milk bank in Christchurch for the parents of small babies.
We’re at St George’s, a private hospital in northwest Christchurch, which provides the Rotary Community Breast Milk Bank with free rent and utilities so it can keep operating. The space, a series of small rooms, includes this room, with several fridges/freezers and a gleaming pasteuriser, a storage cupboard, and a bigger office space where volunteers answer emails and phone calls, and talk to potential donors and the caregivers of milk recipients.
“Even the smallest of preterm babies can digest milk,” says Gergely Toldi, a paediatrician who works at Starship Hospital and at the University of Auckland’s Liggins Institute. Many of them, however, can’t breast or bottle feed because their suck reflex is yet to develop (preterm babies, those born before 37 weeks’ gestation, are often fed via nasogastric tubes). Formula can be harder for preterm babies to digest, as their digestive systems are particularly delicate. While a mother’s own milk is usually the best option, PDM, or pasteurised donor milk, is a good alternative for when mothers can’t lactate for some reason, or if their milk supply is limited or delayed, as can happen when a birth is premature.
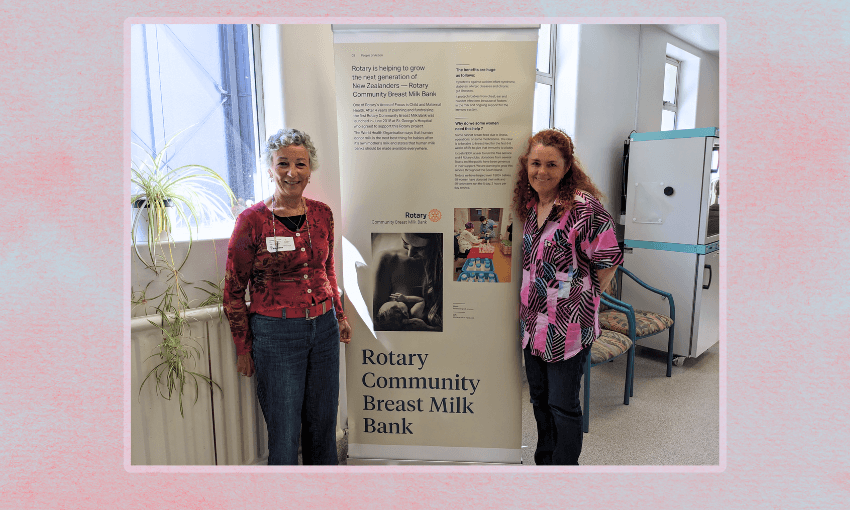
The benefits of breast milk are well known, and even more important for preterm babies, as it contains hormones and nutrients that help babies to develop, and specifically lowers the risk of a gut disorder called necrotising entercolitis. However, there are very few milk banks in New Zealand, with hospital-based milk banks available only in Christchurch, Wellington and Whangārei, and a milk bank run out of a birthing centre in Palmerston North. The Rotary Community Milk Bank is run in addition to the hospital milk bank in Christchurch, as a service for newborns who aren’t in hospital but whose mothers are struggling to produce enough milk to feed them. “The idea was that the Christchurch milk bank would eventually distribute milk to babies in the maternity ward,” explains Yvonne Hiskmuller, a midwife who is chair of the milk bank’s board and a key volunteer. “I was just frustrated at the lack of movement so I thought, why not get Rotary on board and get a committee of people together to establish a community breast milk bank?”
The Rotary milk bank was opened in 2018, and has since provided milk to thousands of babies. Though all the labour, electricity and rent is free, it still costs about $25,000-$30,000 a year to run. “People are happy to buy a freezer, but it’s difficult to get funding for the cost of the screening tests and the pasteurisations and testing the samples,” says Hiskemuller, who adds that each litre of milk the milk bank supplies costs them about $133. This includes cost HTLV blood tests for donors to meet international standards. Money from the Rotary club and one-off grants from companies like Trade Me have helped, but fundraising requires ongoing efforts. “We run sausage sizzles, we sell tea towels, we do quiz night at the pub,” says Lynelle Shemesh, another midwife and volunteer, who has been showing me around. The bank also has an ongoing Givealittle page.
Milk donation in New Zealand is supplemented by a more informal system of milk sharing which may take place in the community, with people who have more supply of milk than their baby needs giving extra to friends or whānau in need. A survey of nearly 500 parents in 2022 showed that 52% of donations were arranged between individuals, and 22% were arranged by hospital staff. Only 20% of donations were facilitated by human milk banks. Health professionals were also surveyed, with almost half of the 232 who answered saying they would like to use donated human milk in their workplace, but access was limited. “It’s a really nice and generous act of sharing milk and helping mums in a difficult position,” says Toldi. “But it’s important to bear in mind that breast milk is a bodily fluid fed to a baby, it can transmit infections even if the chances are low.”
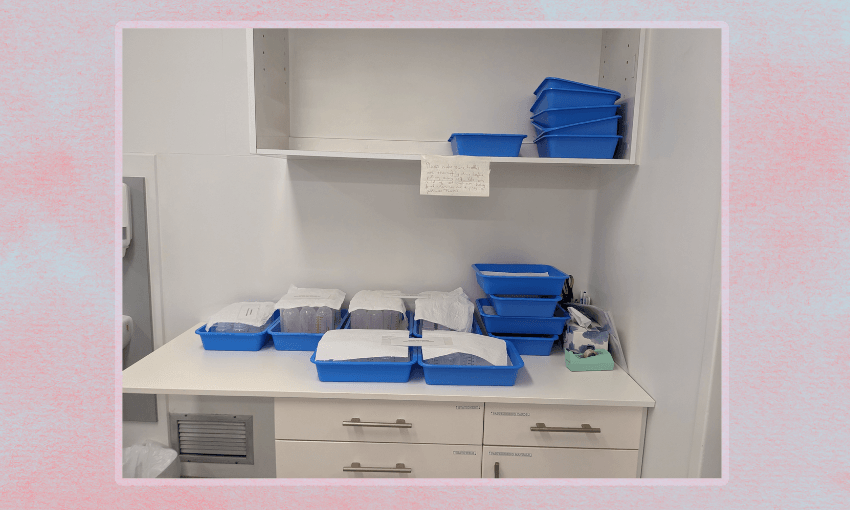
The Rotary milk bank does one-to-one milk transfers; milk from different donors isn’t pooled or mixed. Records are meticulous – there’s a cabinet at the milk bank filled with records and a sign saying that paperwork must be retained for at least 10 years. This means that if anyone has concerns, the milk that has been supplied can be traced back to the donor. As a result, paperwork consumes lots of volunteers’ time; it can take up to 20 minutes to walk a new milk recipient through the documents, and donors go through an interview and blood tests before they can donate.
The people receiving the milk, parents of newborns, are often tired and sleep deprived themselves, yet the space is gentle and welcoming. One of the fundraising tea towels, with a vintage-style illustration of a baby being breastfed, is hung on the wall, and there are lots of informational posters decorating the room, as well as a baby changing table in a corner and a box of empty bottles, returned for sterilising and reuse.
“It’s just been so busy!” says Hiskemuller, half an hour after our interview was supposed to start, sitting down to eat some rice – she’s been too busy to have lunch. Volunteers can come in during the weekends if someone needs milk urgently, and often do more than their rostered hours. “I’m worried about volunteer burnout,” Hiskemuller says; she doesn’t want to ask too much of people. Many of the volunteers are older, although younger midwifery trainees also come in as part of their work experience.
That milk banks are run by volunteers might seem unusual, but all milk banks in New Zealand exist because of dedicated individuals or groups pushing for it. While Auckland is Aotearoa’s biggest city, it doesn’t have a milk bank, although there is occasionally capacity to process milk in the NICU (neonatal intensive care unit) wards of the city’s hospitals. “There seems to be one underlying issue: insufficient investment in timely and appropriate lactation support so families can start off breastfeeding in the best way possible,” wrote Mariana Muelbert, one of Toldi’s colleagues, in August.
This community milk bank exists in parallel with the Christchurch Women’s Hospital milk bank; their volunteers will sometimes pasteurise hospital milk so that neither bank runs out of milk to dispense. The reason this is needed is that the hospital only pays someone to pasteurise part-time. On the whole, though, the milk banks operate independently. That’s in contrast to some other countries, where milk banks are partially integrated with the blood service, as in Australia, or as a network across the whole country, like Brazil, which has more than 200 milk banks. “In the UK and Hungary, where I did the first part of my training, the system was similar to New Zealand, there wasn’t a milk bank unless there had been a local push for it,” says Toldi. “It requires resources to run a milk bank, like with blood – another bodily fluid that needs to be screened, processed and stored in a certain way. This investment is important for longer-term outcomes for the babies, but it requires a financial commitment from the health system.”
Without this commitment, milk has to be rationed. There are strict criteria for which babies can get the pasteurised donor milk, which can fluctuate depending on how much the milk banks have. In the NICU, the criteria is often based on how premature the baby is, with especially early babies prioritised. This criteria might change depending on how many premature babies need milk, and how much supply the milk bank has. At Rotary’s community milk bank, patients are often referred by midwives or lactation consultants. They also occasionally provide one-off donations of a litre or two for mothers who can’t breastfeed after a mastectomy, but had an otherwise healthy birth. In all cases, donor milk can’t be supplied long term – the goal is to get a baby through the first few vulnerable days or weeks until, hopefully, a mother’s supply can catch up.
Brand new babies don’t need a huge amount of milk, just a few millilitres per feed (though feeds are frequent). A poster on the wall of the milk bank shows how quickly babies grow: on the first day of life, 5-7ml is recomamended per feed, about the size of a cherry. By day three, that’s more like 20-30ml, more like an apricot. These small volumes mean that small amounts of donations can make a difference. To give a sense of the scale, Hiskemuller says that in November 2024, the milk bank gave 38.9 litres of milk from 11 donors to 114 recipient babies.
Seeing the sterile, labelled bottles of milk and the steely shine of Daisy the pasteuriser, it’s easy to forget that all the milk that the bank distributes is given, generously, by the parents of small children. These donors have to spend time hooked up to a breast pump when they presumably have a lot of other things to do. “We have fabulous donors, some are very committed with bounteous supplies,” says Hiskemuller. Many donors are the parents of babies who received donated milk who want to pay it forward. “Milk is mainly made by blood, you know,” says Shemesh, still amazed by the process despite working with mothers and babies for three decades.
Outside of this quiet room, breasts are often seen solely in sexual terms. But to Hiskemuller and Shemesh, both working midwives – there’s a moment in our interview when they start describing to each other the births they attended over the weekend – there’s nothing to be shied from in talking about nipples and latching. “You don’t ask, you don’t get,” says Shemesh, explaining how breasts produce more milk to meet a baby’s demand, and gesturing to her chest.
One thing that Hiskemuller, Shemesh, and all the other milk bank volunteers have to be at peace with is the fact that it’s impossible to say for sure to what extent receiving milk will make a difference to babies. “We know that mothers’ milk is more beneficial for long-term outcomes,” says Toldi. “But there needs to be more research comparing mothers’ own milk and donor milk; the pasteurisation treatment impacts the composition of milk, and might mean that the immunological benefits are different even if the nutritional composition is a better match for the baby.” In his work at Starship, he sees how much demand there is for milk, even if the hospital often can’t supply it. “Mums with good supply are keen to offer it to other babies.” According to the 2022 study, 92% of parents supported the use of donated milk in the community, and 98% supported its use in hospitals.
Often, they don’t ever see the babies who are receiving the donation, just their parents. They don’t usually have the capacity to call parents back and ask how things are going after receiving the donation, although they do sometimes receive updates from grateful parents.
As an indicator of demand, two dads come in at 2pm when I arrive, even though the clinic is supposed to be closed to the public. Hiskemuller and Fern, another volunteer, walk them through the paperwork. While the men are quiet, it’s easy to think of the worry that brought them there, a small baby and a tired parent who has just given birth waiting for the precious liquid. Newborn babies don’t need much milk at first, and the milk bank can only supply enough milk for a day at a time. Both men leave with bright yellow cooler bags filled with frozen milk. In the world outside the milk bank, there is new life to feed.