

Alex Casey asks a psychologist why she was too chicken shit to wear a mask during the flight that probably gave her Covid-19.
In the live action replay in my head, I can basically see, frame by frame, the moment that one of those puny little Covid-19 Koosh balls did a Delamere flip right into my mouth. It was last Sunday afternoon, on a stinking hot Jetstar flight about to depart from Auckland to Christchurch, when the lights flickered off, the music dropped out and the wheezy air conditioning took its last breath. The captain came over the loudspeaker to explain that the engine controlling the electronics on the plane had broken, and they needed 10 minutes to pop a new one in.
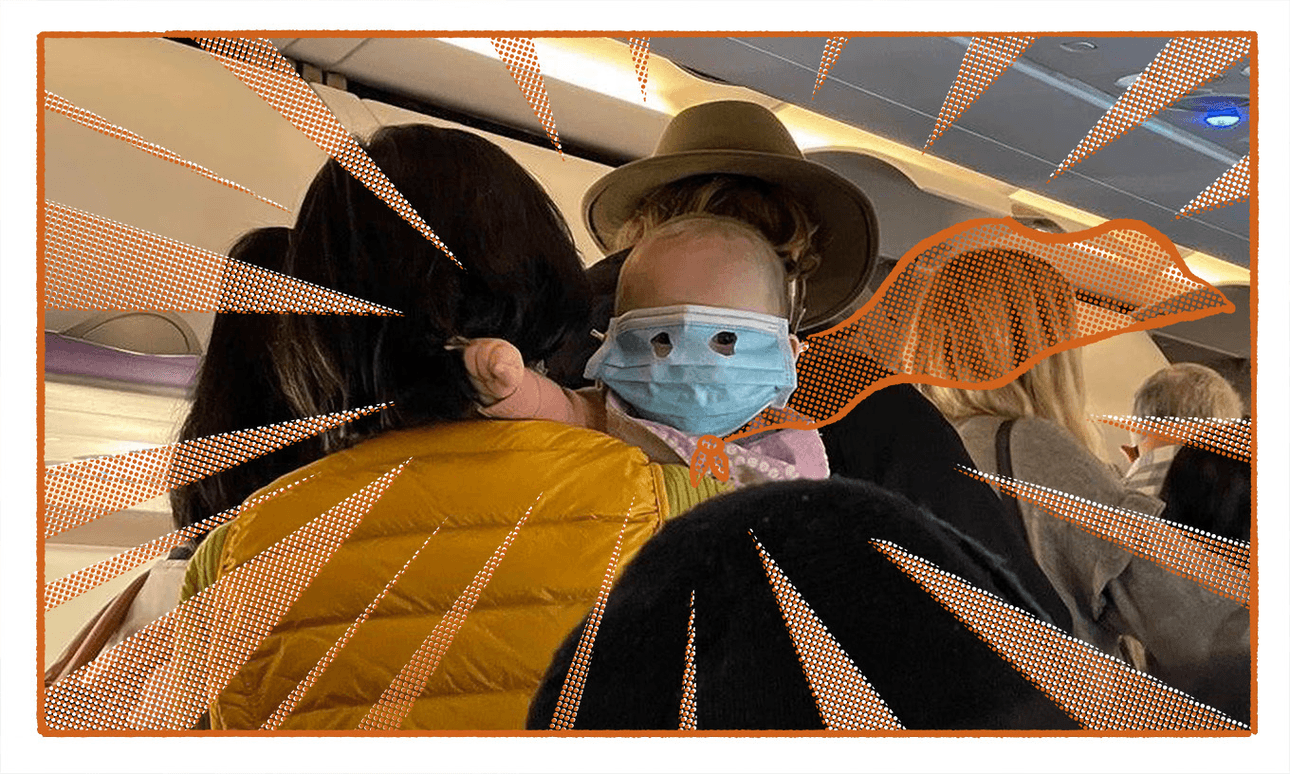
It didn’t seem like 10 minutes was nearly enough time to replace an engine, but this was Jetstar, so I didn’t ask any questions. Instead, I looked around open-mouthed (first mistake) at the festering flight full of people. Much like inside Auckland airport, which was particularly heaving after three massive concerts the night before, hardly anyone was wearing a mask on the plane.
The white guy with dreads in a Snoop Dogg hoodie wasn’t wearing a mask. The pair of sullen lads decked out in black My Chemical Romance merch weren’t wearing masks. The 40 something year-old woman in a Backstreet Boys T-shirt? Clearly not a fan of their 2009 album This is Us because she hadn’t donned a ‘Masquerade’ either. And who can blame them? Masks haven’t been mandatory since September last year – now only required in health and aged care settings – making those who volunteer to wear them feel more or less like total freaks.
Last month I got in an Uber wearing a mask and the maskless driver looked back at me, horrified. “Do you have Covid?!” he yelped. “No”, I said. “So why are you wearing a mask then?” he spat back. An acquaintance told me that her family actually took their masks off during a domestic flight – they were the only ones wearing them, and they felt awkward. At a recent comedy show I went to in Christchurch, a mask-wearer was singled out in the crowd. Although he was praised for his choices, it still felt like a fate just as isolating as actually getting Covid-19.
When I ring psychologist Kirsty Ross, she is quick to reference the famous elevator experiment as an example of how humans are wired to conform, even when it doesn’t make sense. In the 1962 experiment, one person enters an elevator and confidently faces the back wall. Over time, more and more people turned around to face the back wall too. “There are very well established social psychology principles that mean that we are really likely to conform to what’s going on around us,” she explains, adding that there is an evolutionary purpose too. “If we’re identified as still being part of the pack, there is safety in numbers for us.”
Back to the plane. No air, no music, no lights, no masks. Although I had a mask in my bag, I wasn’t wearing one either, paralysed by the idea that I would somehow offend everyone on the plane by suddenly wearing one. Couldn’t simply reach down and put it on now, could I? Wouldn’t want to make a scene and suddenly appear like some sort of ghoulish masked vigilante now, would I? As the stagnant air enveloped us like those green stink lines in Scooby Doo, I instead chose to bravely fall asleep with my mouth open. Not all heroes wear capes, or even masks apparently.
Exactly 48 hours later, I found myself nauseous with a splitting headache, aching bones, a ripper cough and a blocked nose. Covid-19 got me. Again.
Although I could have caught the germ from a range of places during my recent stint in Auckland, nobody else I spent any time with has become sick. I’m no scientist (although I did go to a Wellington Phoenix game with Joel Rindelaub once) but the plane is looking like the primary location of interest. And even if it wasn’t the source, it was still a sealed tube with 180 other people who had all just spent their weekend yelling into the open mouths of tens of thousands of other people. Once again I must ask: why did I not simply pop a mask on, just in case?
“I think the choice that you made was really normal,” says Ross. When faced with an uncomfortable decision in a group environment, she says it can come down to a matter of risk assessment – do I take the long term risk of maybe getting Covid for the next week, or the short term risk of offending my new friend in the Backstreet Boys T-shirt? “There’s lots of things we can say to ourselves to help our estimation of risk to get down to a level where you feel comfortable enough to go along with what everyone else is doing,” says Ross.
It also doesn’t help that Covid-19 is not top of mind for a lot of people anymore, even though 1500 people a day are still catching it, around 200 people are in hospital with it, and around 24 people a week are dying with it. “Now that Covid isn’t really talked about in the news quite so much, and the social messaging around mask-wearing isn’t quite so prominent, it’s harder to make that stance,” says Ross. “Without guidance around what you’re supposed to do, it means the decision is largely left up to individuals now – and those decisions aren’t always easy to make.”

So perhaps next time you’re crammed into a long, sealed vessel with heaps of other people, have a mull over what could be influencing your decision-making. Consider the fact that catching Covid-19 might wipe you out for a week – or longer – and ruin longstanding plans you made with visiting family (sorry Mum). Consider that you might unknowingly pass it onto someone who could suffer a worse fate than not being able to go to the Proclaimers concert (SORRY MUM). Consider… that your decision-making might not even be entirely your own at all.
“This scenario really does show that, as people, we are much more in the flow of what’s happening at a broader social level than we realise,” says Ross, “and our individual decisions are not quite as individual as we think they are.” Now if you’ll excuse me, I feel urgently compelled to walk into an elevator and face the back wall – but at least this time I will wear my mask.

























