



‘All New Zealanders should have equal access to the same standard of treatment’ was the pledge 80 years ago. The data reveal just how far we are from honouring that pledge, explain Carl Shuker and Robin Gauld.
Data analysis and assistance by Alexis Wevers, Vincent Carroll and Catherine Gerard.
Richard Smith, the irascible, brilliant editor for 13 years of the British Medical Journal, one of the biggest and most influential medical journals in the history of the planet, wrote something wonderful in 2011:
“It is not wholly fanciful to compare the Dartmouth Atlas of Health Care with On the Origin of Species. Both books … fundamentally changed our world view. Darwin’s book showed our descent from apes. The atlas exploded the belief that medicine is based firmly on science.”
It turns out healthcare isn’t maths. What Smith was talking about was a project at Dartmouth University in the US by a man named John “Jack” Wennberg. Not a conventional atlas at all. Wennberg’s atlas mapped how healthcare “varies”, and by doing so showed us – not just patients, but doctors – some challenging things. Challenging, in particular, to our perhaps naïve sense that the diagnosis of a health problem implies a treatment or course of further tests that’s basically the same for every person with that diagnosis.
In the US, Wennberg found, Americans were getting different healthcare depending not on what they needed or wanted, but on what was available to be given. You were more likely to get a CT scan if you went to a particular doctor, even in the same practice. You were more likely to get surgery if you went to a certain doctor. Numbers and kinds of tests, scans, surgical procedures, all varied by who was doing the recommending, independently of patient need. In places where more tests are available to be given they were given, regardless of need. One plus one equalled two or it equalled ten, depending on where you lived. This was called “practice variation”. The patterns were “chaotic”.
Well, that’s the US, you might reasonably say: a special case. A free-market healthcare model where healthcare costs more than anywhere on the planet and – shockingly for US exceptionalists – delivers results (including life expectancy) worse than most. Where a course of anti-venom for snakebite might bankrupt you. Where childbirth might bankrupt you. And where the discourse has degenerated so far that Rand Paul (junior Republican senator for Kentucky, and ophthalmologist) can be taken seriously when he says that if you believe people have a right to healthcare that “means you believe in slavery”.
80 years of free, fair healthcare – almost, not quite, or just not
In New Zealand we have a very different, and very special system of public health care. It’s called a Beveridge system, named for William Beveridge, architect of the UK National Health Service (the mighty and embattled NHS). Our public health care is provided by government and paid for with our tax dollars, with a small yet significant private sector for those willing and able to pay.

What’s less known in this country is that our particular and idiosyncratic system was established nearly 10 years before the NHS, which has recently been loudly celebrating its 70th anniversary. Why haven’t we loudly celebrated our 80th? Michael Joseph Savage’s first Labour government passed the Social Security Act in 1938, legislating for the first time that every New Zealander has a right to a free-at-use health system. The 1938 Act had several explicit and farsighted goals that seem eerily contemporary, among them:
- Health care should be universally available and a fundamental right without barriers to access;
- all New Zealanders should have equal access to the same standard of treatment;
- the health system should have a preventive rather than curative focus; and
- services should be integrated not fragmented between primary and hospital-based care.
Passage of the Act met fierce resistance from the New Zealand chapter of the British Medical Association (BMA), the trade union and professional association for UK doctors and medical students. Led by an ex-pat Shetland Island battler named James Jamieson, and against the explicit advice of the UK BMA, the NZ BMA, representing the majority of New Zealand doctors, argued universal access would simply be an unnecessary subsidy for the wealthy and a threat to doctors’ incomes and autonomy. The doctors’ militancy and Harley Street pay-for-play mindset prevailed; to get the legislation passed the Labour government was forced to partially concede.
As a result of this historic compromise, our hospitals are free but New Zealanders pay to see a GP, and we pay even more for after-hours GP consultations. Every increase in the eligible age for free GP visits (now, as of May 2019, 14 years and under) represents a clawing back of those fundamental – and wonderful – goals. The (wildly varying) co-payment for our family doctor is broadly accepted as “how things work.” Out of this historic distortion several oddities flow.
“All New Zealanders should have equal access to the same standard of treatment.” Do we?
The Health Quality & Safety Commission, like similar organisations around the world, publishes an atlas showing differences in the health care New Zealanders get. The New Zealand Atlas of Healthcare Variation is basically an interactive map using data downloaded from all over – administrative data sets that collect hospital diagnoses and treatments, drug dispensing patterns, etc – all encrypted and anonymous, but incredibly useful for seeing patterns and starting to ask questions about why, after you’ve accounted for the different populations living there, different places seem to do things differently.
Hard drugs on prescription
Take oxycodone, for example, in particular that going by the brand name Oxycontin.
Oxycodone is a powerful opioid. The manufacturer introduced the drug to the US in the 1990s with a saturation marketing campaign using massaged and cherry-picked data, more than 20,000 “educational programmes” for physicians, “starter coupons” to hook patients with a free seven to 30-day supply, plus junkets and other forms of soft power to incentivise prescribing especially by primary care doctors (including branded swag, like Oxycontin teddy bears and a CD of ’50s dance music called “Get in the Swing With Oxycontin”).
In 2007, Purdue Pharma, manufacturers of Oxycontin, pleaded guilty to federal charges that they misrepresented its potential for addiction and abuse and paid the highest fine ever paid by a big pharma company: US$600 million. In the meantime, however, oxycodone had sneaked into New Zealand on the back of that marketing push and between 2007 and 2011 our oxycodone prescribing rates more than doubled even after Purdue copped to the charge.
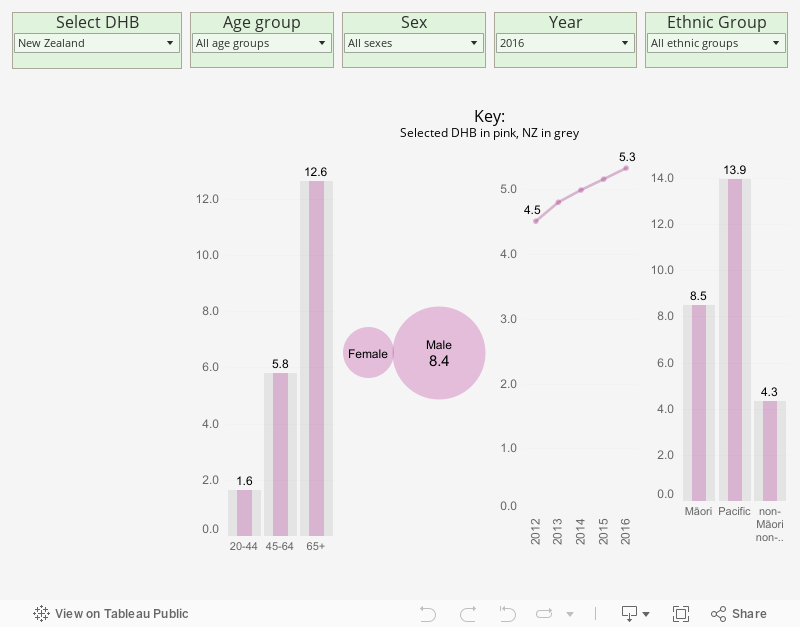
The Atlas of Healthcare Variation shows the number of people picking up strong opioids (fentanyl, methadone, morphine, oxycodone and pethidine) from their pharmacy on a consistent increase in New Zealand, from 14 people per 1000 in 2011 to 17 per 1000 in 2016. That’s 77,000 New Zealanders in total in 2016.
But behind this increase are some interesting idiosyncrasies. In 2016, 11 people in every 1000 in Capital & Coast DHB got a strong opioid at their pharmacy. In the Bay of Plenty it’s more than double that rate (nearly 25 in every 1000) and climbing (1400 more people since 2011). Not far behind the Bay are Northland, Whanganui, Wairarapa, Hawkes Bay, and Nelson Marlborough. Scroll down and click on your DHB to find out the rates where you live.
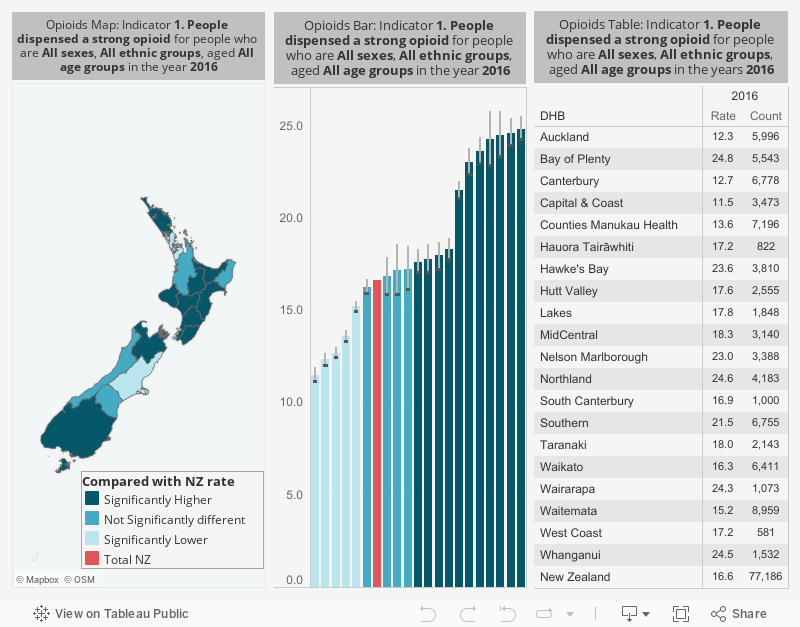
If the chart above fails to load, please turn off your ad blocker or alternatively view it here
Just as depending on where you live you’ll pay more or less for a visit to a GP, depending on where you live you’re more or less likely to get a very strong and very addictive drug for pain.
So who’s on those opioids? In Bay of Plenty, as in most of New Zealand, we can see from the bar graphs below, it’s mostly older white people (12% of those over 80!), both men and women.
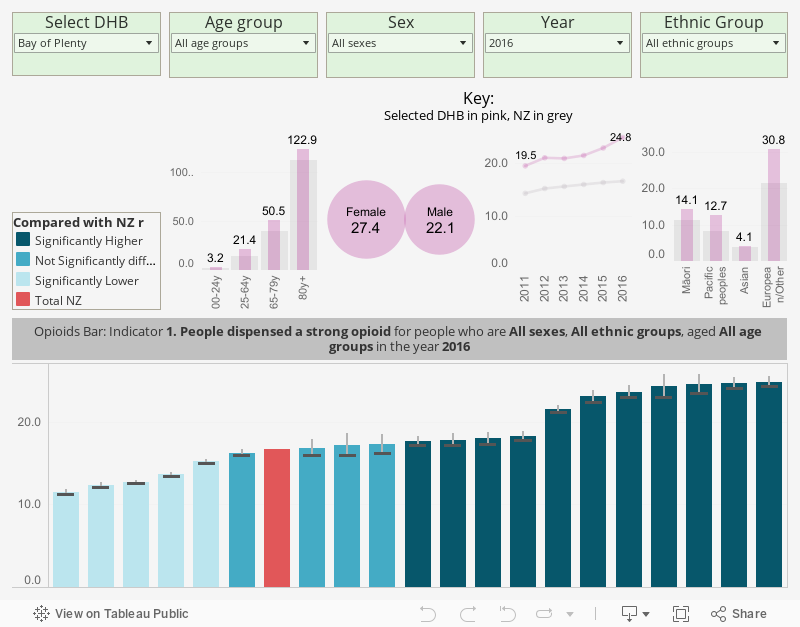
If the chart above fails to load, turn off your ad blocker or view it here
Oxycodone is a slightly different story to strong opioids generally – as word of the dangers has spread (however late), oxycodone dispensing rates across New Zealand appear to have decreased.
But take another look at the graph below. Although the decrease is primarily in those most using opioids (i.e. Europeans, in red), Māori, Pacific and Asian populations (blue, green, and orange respectively) are still being dispensed oxycodone at the same or similar rates as five years ago when the dangers finally started to go public here.
Prescriptions of an addictive, dangerous drug to Pacific people has even slightly increased. How can that be explained?
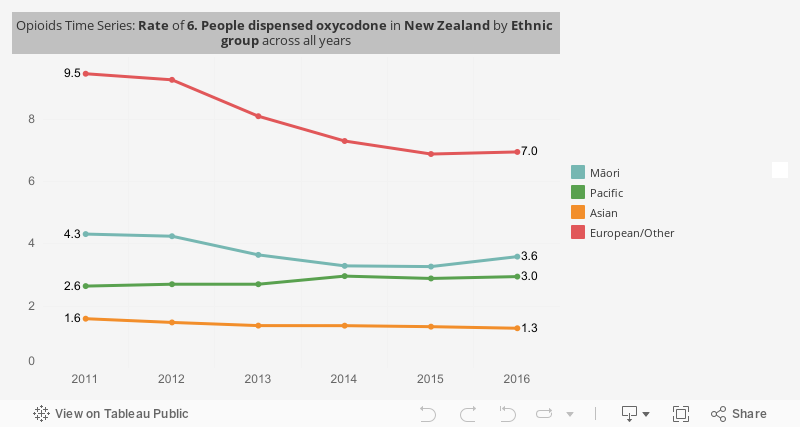
If the chart above fails to load, turn off your ad blocker or view it here
Tonsillectomy and the sound of music
Variation is not always so obvious and explicable. Early on in his investigations of variation, Jack Wennberg found two little towns in Vermont state called Waterbury and Stowe. (Leafy, rural Stowe’s famous for being the town in which the Von Trapps of The Sound of Music settled when they came to the US in the 1940s.) These two towns were about the same size, 4,000-5000 people, and only 16 kilometres apart, but behaved quite differently in their healthcare.
Wennberg found that by age 15, 60% of Stowe children had their tonsils removed, while just down Route 100 in significantly less-famous Waterbury, only 20% of children did.
Tonsillectomy in children is no joke – surgical removal of tonsils for sleep-disordered breathing or repeated tonsillitis requires a general anaesthetic in children, with all the risks, costs and discomfort a general anaesthetic entails. Why would six of the ten Von Trapp kids have their tonsils removed rather than only two, depending only on a distance of 16 kilometres? (Would there have been a Sound of Music with eight more tonsils?) Why were doctors doing things differently, and patients choosing differently, in towns otherwise fairly similar and only as far apart as Ponsonby and Ōtāhuhu? (And does that analogy start to suggest a possible answer?)
Tonsillectomy is what is known in the language of variation as both supply-sensitive and preference-sensitive – if parents decide it’s a good idea (versus watchful waiting) based on what their doctor recommends, it happens. One ENT specialist can make a big difference to a smaller region. In New Zealand, tonsillectomy rates are significantly higher in non-Māori/non-Pacific people compared with Māori and Pacific peoples. They’re significantly higher depending on where you live. Depending on the DHB catchment you live in (South Canterbury for example) your children under 14 are three times more likely to have the operation. Can both ends of the spectrum be right at the same time? Who’s choosing? Who’s deciding?
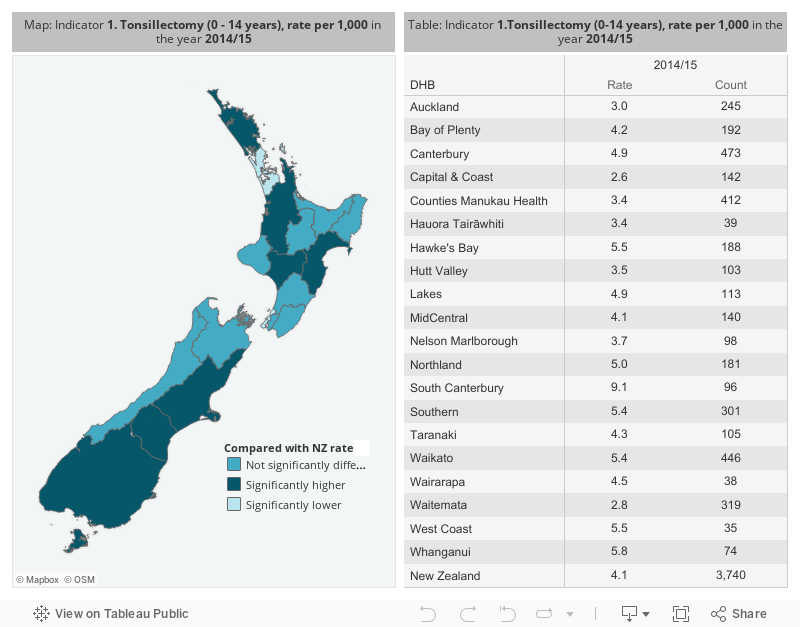
If the chart above fails to load, turn off your ad blocker or view it here
How do dollars for doctors affect the healthcare we get?
Some of us don’t get the healthcare we need, or we get it too late – which is the hard, expensive end of acute hospitalisation for conditions that should have been treated by a GP long ago.
Asthma
Generally, asthma sufferers use two kinds of inhalers: a reliever (for emergency relief for an attack), and a preventer, for those using a reliever more than twice a week for asthma attacks. Asthma under good control would be characterised by little use of relievers and regular use of preventers, and thus low numbers of hospital visits for asthma attacks.
However, the data show 32% of people regularly dispensed reliever medication at a pharmacy were not regularly dispensed preventer medication. One in five were not dispensed a preventer at all.
The results of this uncontrolled asthma are a hard end: acute hospitalisation. First of all, very young children are much more likely to be hospitalised for asthma than older children or adults. About 5000 New Zealand children were hospitalised in 2016, and about 2000 adults. Pasifika children are more than twice as likely as Pākehā children to end up in hospital with asthma. When it comes to adults it gets worse – Māori and Pasifika are more than three times as likely as Pākehā to end up in hospital for asthma. Nearly a fifth of those admitted to hospital were back in hospital at least twice in the year following, and over a third didn’t then get preventer medication from a pharmacist. That is uncontrolled asthma acted out over a system.
Gout
Gout is another one. It’s a much misunderstood condition arising from build-up of uric acid in the joints, and one characterised by a nasty trifecta of high prevalence, victim blaming, and inadequate treatment at primary care level. Gout in our culture is usually attributed to over-indulgence in seafood and alcohol, met with a snigger or sense of resigned inevitability. But here’s how an anonymised self-employed Samoan father in his 40s in a recent study describes it:
“I can’t hack the pain, but I need to go pay these bills. If I go to this clinic, no one’s going to go pay the bills. Or I can hack the pain, and go to work. And if I don’t hack the pain, and I don’t go to work, my family doesn’t eat.”
Gout is in fact a treatable form of arthritis, one that causes excruciating pain that sufferers are implicitly or explicitly told to live with, as if it were their own fault, and as if changing their diets and drinking could alter their uric acid levels more than just 10%.
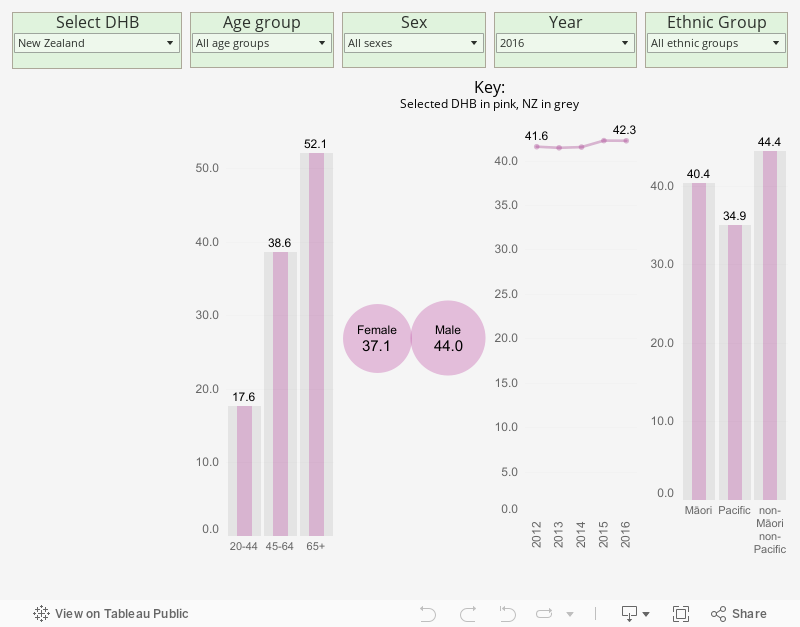
In New Zealand the data reveal the massive numbers of people identified with gout – 5% of the population, or 182,000 people (nearly 28,000 people in Counties Manukau DHB’s catchment alone). Nearly half of Pacific men over 65 have gout. Compare those bars in the graph below for ethnic group.
If the chart above fails to load, click here
The intense pain of gout arthritis (“It felt like my foot had been run over by a car” is how one 28-year-old man describes it) is quite controllable through what’s known as “urate lowering therapy” – drugs that lower the uric acid in the blood, like allopurinol, prescribed by a GP. But people aren’t getting it. Atlas data show that less than half of New Zealanders with gout are regularly getting the right drug.
And again we see the hard end – expensive, distressing, acute hospitalisation (nine times higher for Pasifika and four times higher for Māori) for a condition that can be treated by a pill a day on advice from your GP. How much pain do you have to be in before you go to an emergency department?
Click on your DHB to find out how many people are regularly receiving urate lowering therapy where you live.
If the chart above fails to load, turn off your ad blocker or click here
The system we never got
The goals of the 1938 legislation were never delivered upon due to that historic compromise with the NZ BMA, and the impacts on us have been widespread.
People who need elective procedures have different access depending on where we live and our ability to pay. Particular DHBs are considerably better placed to meet demand for electives; others will not receive referrals from GPs as they will be unable to deliver in a timely way. People with private health insurance can get their electives in the private sector where, in areas such as orthopaedics, more than 50% of procedures are performed, often by the same specialists who work both the public and private sectors. Private prices vary around the country. Many patients will simply pay personally for private service and receive rapid access to treatment as a result, and perhaps a referral back into the public sector, thereby jumping the public sector waiting list for what’s known as a “first specialist assessment” – where a specialist assesses a patient’s needs against national criteria. Studies have found that these clinically agreed criteria can be gamed by patients and specialists, increasing the score a patient is given and therefore improving likelihood of receiving publicly funded treatment.
In the primary care and general practice sector prices around the country vary greatly. Again, geography plays a strong part as some regions receive more government funding than others. A wealthy person can pay much less to see a GP in one area than a less-well-off person in another.
Money is a barrier to healthcare in New Zealand, it shouldn’t need repeating, but the data show it.
Statistics NZ data show over 14% of the population attributed cost barriers to unmet need for healthcare, rising to 20% for those living in the most deprived areas of the country.
The Health Quality and Safety Commission’s large national patient experience survey shows cost barriers disproportionately stop Māori and Pacific people from seeing GPs and getting medications. Nearly a third of Māori (28.7%) and Pacific (29.3%) patients responded that cost stopped them visiting a GP or nurse, compared with 18.5% of European patients. (And this is within a cohort that had already accessed a GP.) Nearly a quarter of Māori and 22% of Pacific patients said cost prevented them picking up a prescription, compared with only 7% of Europeans and 15% of other ethnicities.
It’s not just money. Māori adults were less likely than Europeans to answer yes to the question “Was the purpose of the medication properly explained to you?”
The multiplier effects are hard to measure but the logic of attritional grind is brutally clear: fewer people attending a GP, fewer of those who do so then actually picking up their prescription, and a significant number of those few then not understanding their medication once they get it. Just as brutally clear is the fact that nearly one in five of the most advantaged population in the nation still won’t go to their family doctor because of the cost – in egalitarian New Zealand where universal access is enshrined in law.
Advocates of the current system may say we now have free access for under 14s. But one of the collateral effects of historical financial barriers to access is the force of habit and the intergenerational transmission of knowledge – some New Zealand families simply have no tradition of a family doctor. Their tradition is sticking it out until you need the emergency department.
The Simpson Review – a chance to put things right?
Attempts to forge better integration of providers in the health system – in essence, primary care and public hospitals working together as part of one health system – aren’t easy. This is mostly because public hospitals and primary care are funded quite differently, with very different income and incentive structures. Broadly, public hospitals receive a fixed income out of which they pay staff salaries. Primary care and general practice are privately provided, with around half of income from a mix of government sources, and patient co-payments making up the rest. A book could be written on the fine details and still not fully describe the nuances of different regions and arrangements.
The result of this complexity means patients and providers are often involved in multiple work-arounds as they intersect with different systems and processes. The transaction costs – the administration involved in supporting an over-complicated system compensating for its inbuilt distortions – are not insignificant either.
How might the system be better designed? The health minister’s health system review, named “the Simpson Review” after chair Heather Simpson, is presently deliberating. It will need to provide some answers and there are many possibilities. To reduce some of the anomalies and inequities in our system could require increased funding injections to ensure that no patient faces financial barriers. Why should a patient not be able to see a GP due to a fee for service? Why should it be acceptable for those of better means to go private, rather than wait in line in the public sector? Debate is required over everything from employment arrangements in the hospital sector, to how to reduce or get rid of general practice charges forever.
Eighty years on and straying from the path
Healthcare varies. It moves as you play, it changes with the skin colour of the player. There are almost unlimited examples, many stemming from that seminal 1938 distortion in our access to a local family doctor.
Variation is a measure known as a ‘can-opener’ – it’s not always a dial where high is bad and low good. It’s a tool that opens a can of worms and poses a lot of questions. Our healthcare system is large and unwieldy and the questions raised are sometimes complicated, but they are important, often urgent, and often obvious.
Last year was the 70th anniversary of the NHS, which means this year is the 81st anniversary of the NZ Social Security Act and our amazing healthcare system. We sometimes do world-first stuff despite a tiny population. Put more modestly than that, but perhaps of greater weight, New Zealanders can simply routinely expect care that is first-world, and that’s all the more impressive given the economies of scale we lack. All of that. The problem is only some of us can. The law says our healthcare should be “universally available” and is a ”fundamental right,” and that everyone “should have equal access to the same standard of treatment.”
These are worthy goals and right, but it’s been apparent for a while now that in practice our healthcare is not universally available and people do not have access to the same standard of treatment. As the system turns 80, it’s well past time to have a hard look at who exactly has cause to celebrate.
Robin Gauld is Pro-Vice-Chancellor (Commerce) and Dean of Otago Business School. He is also Co-Director, Centre for Health Systems and Technology at the University of Otago. Carl Shuker is the author of A Mistake and principal adviser in publications at the Health Quality & Safety Commission, but the views here are his own























