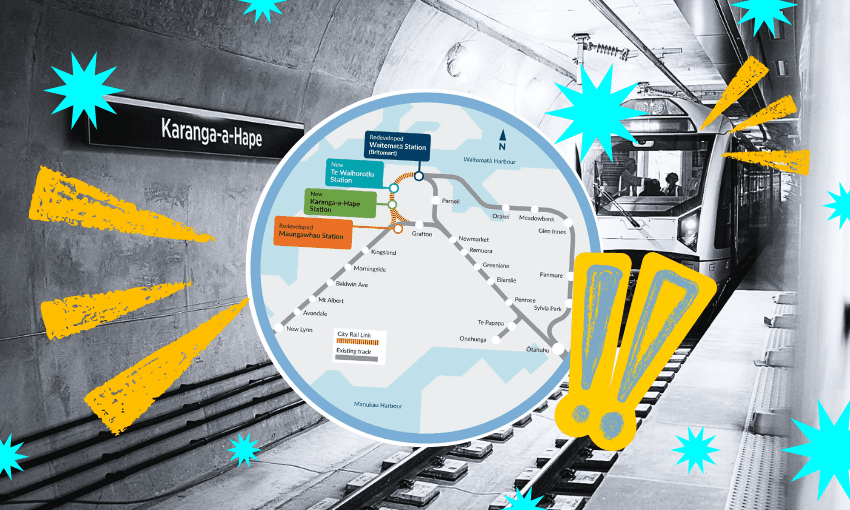



Even before the dust has begun to clear from the Covid crisis, DHBs will disappear, replaced by a new national health service and Māori Health Authority. Toby Manhire meets the leaders, Margie Apa and Riana Manuel.
When you tear open the envelope and fish out your voting papers for the local elections in a few months’ time, something will be missing. There will be no list of assorted experts, concerned citizens and cranks seeking an elected place on a district health board. Because there will be no district health boards. Last year, two decades after a Labour government introduced the system that sliced the country up into 21 – and later 20 – regions, another Labour government announced its abolition. On July 1, the ribbon will be legally cut on a new, massive agency to replace them all, provisionally called Health New Zealand, with the Māori Health Authority alongside it.
The sheer scale of the new organisation and the magnitude of the overhaul are colossal. DHB bosses variously described the change as “an atomic bomb” and a “tectonic shift”. The new agency will be the biggest employer in the country, with a workforce of around 80,000 and an operating budget of something like $20 billion a year. It inherits long waiting lists, limping infrastructure, an overstretched and exasperated workforce; a system bedevilled by fragmentation, regional imbalance and inequities – for Māori especially – that have spread through pretty much every cell of the body.
It’s a lot. “Oh, it’s huge,” Margie Apa says, matter-of-factly, on a Zoom from Wellington. “It’s huge. Once in a generation.” Apa is CEO of Health New Zealand and sitting to her left is Riana Manuel, CEO of the Māori Health Authority. They’re just a few weeks into their roles, but as far as it’s possible to tell through the screen of a laptop, the rapport is strong. They’re already finishing each other’s sentences. When I point that out towards the end of the interview, Apa says: “I brought breakfast, she brought lunch.”
This seismic change in the way health is run across New Zealand comes as the system convulses still from the unprecedented challenges of a pandemic. Both women saw it happen in close-up. Apa was until recently CEO of Counties Manukau DHB, which includes New Zealand’s most Covid-burdened hospital, Middlemore, as well as leading the northern region’s response to the pandemic.
The Counties Manukau job was close to Apa’s heart: she was born in south Auckland, her parents having arrived in New Zealand as part of a wave of migration from Samoa. In the 80s and 90s the factories and freezing works that employed so many of the new New Zealanders closed their doors. “Places like South Auckland really suffered,” she says. “The really visual image for me, growing up in a community where you see young men who had been working, who were strong … your peers and fathers of your peers. It was very visceral for me, seeing young men lose track, become mentally unwell, whole families really suffering from that. I was really fortunate to have had parents and a large extended family – we kind of supported ourselves through it.”

Manuel (Ngāti Pūkenga, Ngāti Maru, Ngāti Kahungunu) grew up in the small Coromandel town of Manaia. Her mum was (and still is) a nurse. At one point her mum was the nurse on the ambulance, her dad the driver. “She was a district nurse, she was a public health nurse, she was the Plunket nurse. And she was also the home-based support services. We were always part of that. She was a rare kind of commodity in our village.” The family phone rang off the hook. “And I watched her navigate and create, if you like, a locality kind of system” – localities are central building blocks in the new system – “in our little village. I think that’s what’s prompted us to all go on and do what we do.” Her brother trained as a nurse, then went on to become a surgeon and is now a GP. Riana became a nurse, took on leadership roles and most recently led the iwi-based Te Korowai Hauora o Hauraki and the Hauraki Primary Health Organisation.
“What I also became aware of at a really young age is the inequities around Māori health,” says Manuel, leaning forward, face mask dangling from her forearm. The most bald and shocking data point in New Zealand health is that Māori people on average die seven years earlier than non-Māori. You didn’t need the statistics to see it. “Just, you know, noticing that I was always at tangi. And those tangi were generally for people somewhere in the region of 40 to 60 years of age. When you grow up seeing that, and you start to realise in the bigger ethos of health there are some things that are really playing into that, it got me interested in Māori health. So I’ve spent the majority of my career working in community-based and Māori health kaupapa trying to, you know, turn the dial. When I started nursing, that was the time of the last reform, and when this opportunity came about I thought, you know, it’s one of those moments when you think to yourself: ‘This could be a game changer. Let’s give it a good go.’”
Hauora Māori
Like a film of snow on a landscape, Covid-19 freshly revealed many of the known failures of the system. It was disjointed: a jumble of overlapping, ill-fitting pieces, a mishmash of information technologies. And it was unfair: a set-up where some groups of people routinely got a better deal than others.
The Waitangi Tribunal’s Wai 2575 Inquiry had already set out the state of health for Māori; last year, an urgent tribunal report on the Covid response was damning, identifying equity failures and treaty breaches. The Māori Health Authority, with Manuel at its helm, is designed to address both of those.
How will she ensure that her body does not become subordinated to the bigger beast? “I think like all good partnerships you’ve got to make sure that you’re always relevant and ever present in the conversation,” she says. “I think the legislation will set out some of their clarity, but what we aim to do at a leadership level is to make sure that every conversation is inclusive of that thinking. Te Tiriti is a separate conversation to equity but we need to make sure that those foundations are there in order to drive through those projects, and those kaupapa, that will address the inequities that exist.”
Hauora Māori must not be just some bolt-on, says Manuel, but “at the heart of what we’re doing”. And to the idea that the solution to the health predicament of Māori is individuals taking greater responsibility for themselves, Manuel’s rejoinder is this: “Self-responsibility occurs once we have an equal playing field.”
For Apa, the decision to go for the job was “seeing that the government looked pretty serious about addressing inequities”. She says: “No health professional should look at our stats for Māori health for the fact that that’s OK. So the only answer is really to have Māori take a much greater stake and input into how that happens at all levels of our healthcare system.”
The parts of New Zealand that have been under-served by the health system over decades don’t stop at Māori. Whether it’s Pasifika, rural and remote populations or disabled communities, the health experience has too often fallen short – can they expect better from Health NZ?
“You’ve had frontline experience,” says Apa, nodding towards Manuel, “of how it works when the system allows communities to be involved and resourced in a way that suits them best. And I think that’s one of the challenges of our current system, is that we fund as if there was a one-size model that fits everybody.” The days of tinkering are numbered, she says. “We’ve got to cut through that and get straight to the core design, and start from the beginning: what’s going to reach those communities? It will look different across the country, because it should.”
Health, in its full, true sense exists well beyond the bounds of clinic or hospital walls. “The social determinants of how we create healthy environments have to come into the picture as well,” says Manuel. “Really good respiratory care comes from living in really nice, dry homes that are fit for purpose. So we want to have good partnerships with Kāinga Ora. We know that disability communities have very real needs, functional needs that mean that they can get out into their communities. How do we make sure that that’s happening? Working with everybody across sectors: education, justice, looking at different ways, different models that will suit different people.”
The pandemic, again, has been instructive. “Covid has taught us that you actually get very little done when you tell the population to come to you,” says Manuel. “What is more effective is when you go to the population, so all those little vans, those carparks, those marae that have been working for the last two years to make those systems work, we want to galvanise that and make sure that we invest in those spaces.”
Apa picks up the thread. “Those models have always been there, but they’ve been seen as on the fringes, as boutique. The providers have tried to deliver them where they could cobble together the resources. What we saw over Covid is they actually need to be more central to the way that we deliver care and services normally. Because when we did resource it, it got the populations out.”
Manuel again: “A pandemic is an opportunity to learn. You have two leaders here who have literally been in the front of their organisations and the responses, and have seen those learnings firsthand.” Before Covid, she was delighted to have six general practices across Te Korowai Hauora o Hauraki catchment. “But nothing got us as close as getting into local RSA carparks or the marae. We got much closer to the communities that way. And not only did we take Covid testing and vaccinating with us, but we did diabetes screening at every single car that went through. And we found so many people who we had to refer on to specialist services, because they were literally unaware that they had these really exacerbated blood sugars.”
The shift in thinking is epitomised in the questions she sees on Te Korowai’s Facebook page. “People are constantly going: ‘Where are you guys gonna be next weekend? Which part of the peninsula are you coming to?’.” When those questions, and the bigger policy questions behind it, are answered, when it works, the idea is that the new framework will be able to replicate the response around the country. “An exciting part of being HNZ is that we can coordinate the spread of that kind of approach much quicker,” says Apa.
A workforce at breaking point
Wherever you look across the health system, its people are shattered. A stream of industrial disputes – most recently a strike planned for last week that was blocked by the Employment Court – are as much about conditions as they are pay. A government-commissioned review of nursing capacity recently found that one in four shifts are understaffed. Half of the 2,100 respondents to a survey of senior New Zealand doctors by the Association of Salaried Medical Specialists last year said they were experiencing “high levels of burnout”. Responding this week to the announcement that Covid-positive staff can return to work, Kerri Nuku of the NZ Nurses Organisation told RNZ her members were “angry and frustrated, they’re burnt out, they’re tired and fatigued”.
I spoke to half a dozen health sector employees before meeting Apa and Manuel. Most were cautiously supportive of the reforms, but amid the various concerns they raised, the one common theme was staff strain, exhaustion and morale. I put that to the new leaders, together with the summary of one health worker: “People feel like they’ve been treated like shit for decades.”
“Yes,” says Apa. “And we are going to be thoughtful about the pace of change and not be tone deaf to the pressures that people have. Unions are a really important sounding board for us, they will tell us very quickly if the members are saying this is not working for them.” While the Covid crisis had “exacerbated a lot of the issues that we see today”, she stresses, “they were already there before Covid.”
She is frank about the workforce shortage. “We do not have enough health workers and we need more. We need to be investing in our workforce to develop the skills that they feel can add value to the care they provide. And while we won’t solve that overnight, it is important that we are engaging our clinical leaders, our workforce leaders to be part of problem-solving our way [through] … And it’s important that we are actually thanking our staff – I take every opportunity to acknowledge that our teams are working in incredibly tough environments.”

Connected to that, she says, is a shortage in capital investment, which “actually creates the workplaces, or makes available the digital technology to give people the tools to do the job better. And so again, as one organisation, as one system, we can unify the process and be transparent and simplify how we get capital investment into the country, so that our workforce can see that we are seriously investing in them.”
Some argue that the strain on the workforce and the system across the pandemic makes this precisely the worst time to tear it up and start again. Manuel disagrees. “I know, having been out there with my teams, every weekend, every day on the frontline, that it’s hard work. It’s relentless, you don’t get breaks. If you’re feeling undervalued, the message from us is that the whole reason why we need a reform to happen right now is to make sure [we respond to] people who don’t feel heard, who don’t feel valued, who feel marginalised. I hear a lot: ‘Why are we doing this while Covid is here?’ Well, you’ve just articulated for us why we need to have the reform. Because something needs to change, a lot of things need to change. And that’s what we aim to do.”
If you were marking a halfway point between now and that July 1 starter pistol, you’d plunge it into May 19, budget day. For their ambitions to be realised, does the government need to – forgive the image – cough up?
Apa draws a diplomatic breath. “We’re all looking forward to budget announcements soon. But, certainly, I don’t think there’s any denying that the system does need more investment and resources. And it’s a matter of really just supporting the government to make those choices. When we’re all separate entities, it is quite tough for the minister of health to try to present our collective view of what the system needs, because we all put up our own individual DHB bid … But these are tough choices and tough times for the government. So we’ll see what happens over the next few weeks.”
“You know,” says Manuel, “we want to make sure that we’re getting the best efficiencies out of those dollars. But every year, year on year, we’re going to have to invest in a transformation. Otherwise, you’ll just roll over what you’ve got, it won’t change, it won’t alter. So, yeah. We’re looking forward to budget day.”
The mental health crisis
The 2019 budget saw a record spend in mental health, with $1.9m earmarked to power up an over-subscribed, struggling and sometimes shambolic branch of the health system. Almost three years on, despite government assurances that progress is being made, there are few signs that a corner has been turned. That, too, is in large part down to staffing, says Apa.
“Workforce is at the heart of much of our challenge in the sector. We don’t have enough psychiatrists. We don’t have enough psychologists. We try and expand talking therapies, counselling – that’s really central to opening up access to those referred by a general practice. That’s a really critical rate limiting factor for us.” There had, however, been programmes in parts of the country that had succeeded in widening availability, she says, pointing to the northern region, and those examples could be replicated elsewhere. “We need to do some very, very fast focused work on just growing workforce and trying to work out how we shorten the training time for people to get into these professions, and still have some supervision of what they do until they become fully grown as professionals.”
Manuel returns to the challenge beyond the formal system. “Mental health is another chronic condition, whereby lots of things lead to these kinds of outcomes – poverty, education, all of these factors,” she says. And in an area that is “super important to the Māori Health Authority”, the model needs to be tailored to those affected. “One size fits all is not going to cut it here. What happens for our rangatahi is very different to what happens to our 20 to 40-year-olds, for instance, and the kind of social and mental health needs that a 50 to 80-year-old has are very different again. I’ve seen some amazing outcomes out in small communities, where they put into practice even just the smallest of things … There are lots of different things we could try.”
What does success look like?
The health system is a tanker. It takes time to switch direction. But some changes should be apparent fairly quickly, says Apa. “If we’re doing our job, it’ll be in the first year.” She offers the example of someone awaiting a hospital procedure. “I think people might be a bit surprised to find, if you’re in south Auckland, your hospital might say, actually, we can’t provide it for you at Middlemore, but would you like to go to North Shore and get it done within a week or two? And I think that will be telling our community that we are working as one unified system, and we’re offering our community access to services across the whole region, not just being constrained to what’s available within their own district health board.”
Over time, something similar might happen on a wider scale – and flipped so the health professionals are the ones moving around. “If we’re really doing well, we might have teams of people who might fly out, for example, to Tairāwhiti to clear a list of cataracts. It means thinking less about only serving our local population, and thinking more about what’s the best thing to do for people, about bringing the resource to them if that’s required.
“While still always being mindful,” adds Manuel, “of those equity challenges.”
“Ultimately the prize,” says Apa a few minutes later, “is that we see people living longer lives, particularly Māori, who have a lower life expectancy. Commentators might think it takes a long time to effect but actually if we unpick what contributes to shorter lifespans, much of it is within the control of the system.”
For Manuel, there are twin challenges: transition and transformation. In the course of the transition that is coming, she says, they’re determined to keep their eye on the lodestar. “We need to make sure we’re always looking to what we call te pae tawhiti, the horizon, the destination. We want to make sure that we’re reaching towards that, setting out our goals and starting that navigation, so we don’t just focus on the system we’ve got, but: what is the system we want? And how is that going to look?”