A full 50% of the population will experience menopause, but confusion about its symptoms – and the options for treating them – remains widespread. Determined to address menopause’s debilitating effects, Anna Sophia embarked on an ‘experiential trial’ to discover whether hormone therapy could help.
So here it is and here I am. Fifty-seven years old, late to the party, I’m finally experiencing menopause.
I have no idea why I am just rocking up to the most major transition in my life. Genetics perhaps, or maybe my second child arriving when I was 43 tricked my body into believing I was still a young woman.
At 56 I was having regular periods, although in hindsight other symptoms had emerged over the previous years which I had shrugged off as age-related wear and tear. By then my days had begun to structure themselves around eating cake. Kilos attached to my waist. By the way, the Sugar Plum Café has superb carrot cake if you’re passing through Marton.
I didn’t realise my oestrogen levels were a dripping tap.
There’s a pervasive silence surrounding the most major transition that women make. A million or so women over the age of 40 living in Aotearoa are either heading quickly toward menopause or living through this seemingly never-ending transition.
As a practising counsellor (MNZAC) for 25 years, I have listened to many women’s stories. I have been the director of a nonprofit counselling organisation for 21 years. I have a degree in social anthropology and women’s studies and a long-term interest in women’s health. I read widely and extensively.
This is what I knew about menopause: NOTHING.
If before my own menopause, I thought about it at all, and I really didn’t, this is what I thought would happen: I’d have a few hot flushes, my periods would stop, and I would just carry on feeling the same as always. Ask any menstruating woman what she thinks will happen and I can almost guarantee she has no idea.
Society is now discussing many things that were rarely talked about until recently. Mental health has made its way out of the closet. The #MeToo movement is growing stronger by the minute. My rainbow teenager and friends stroll confidently through the world as their full colourful selves.
Menopausal women still live in silence, in the margins.

My symptoms appeared three years ago. Alongside the cake addiction I found myself gradually losing joy and desire. I wasn’t depressed, but there was no variation of emotion. Life became a monotone blank. I missed feeling joy but I also somehow missed my premenstrual rages where I wanted to chop someone’s head off.
Life lost the multifaceted cyclical rhythm that I had lived by for 40 years. It didn’t matter how much I exercised, how many vegetables I ate or how much I gazed at my expanding navel, nothing changed. I was stuck on a joyless trip to nowhere.
The predicted hot flushes came and went but they didn’t really bother me. It was the symptoms I didn’t know were related to menopause that floored me.
My hips ached after walking small distances and hurt at night as I tried to sleep. An avid hiker, I now felt my knees ache when I walked down hills and steps. Getting out of the car was an effort and it took ages for my body to recover from a short car ride. My shoulder ached for months.
I woke six times during the night to go to the toilet but found I didn’t really need to go. Then I couldn’t get back to sleep. I had heart palpitations most days and low-level anxiety.
I embodied fatigue. Thinking about what to wear each day was too hard. Black track pants and black tee shirt were my uniform. Cooking from a meal kit delivery was too exhausting so I bought ready-cooked meals in bulk. Fridge or freezer to microwave. Containers straight to the trash. My once sharp brain was engulfed in a chronic fog and I could no longer think clearly.
Like menopause itself, I also knew nothing about menopausal hormone therapy (MHT, often referred to as HRT, or hormone replacement therapy), except that it apparently could cause breast cancer or heart disease – or so a hugely influential women’s health study told us when it basically wiped MHT off the map in 2002.
So I was in for a surprise when I joined 200,000 other women on the forum of Balance, an app for menopausal women created by leading UK specialist Dr Louise Newson, whose invaluable website and podcasts I can’t recommend highly enough. I learned that MHT is not the big baddie after all and menopause specialists are now advocating its use as a preventative especially for osteoporosis, fracture risk and heart disease.
That last one is particularly striking, given the longstanding belief – even among many doctors – that MHT actually increases your risk of cardiovascular disease. However as the Australian Menopause Society puts it, “Numerous studies have shown that, in women under the age of 60 years with symptoms or other indications, initiating HRT [MHT] near their menopause provides a favourable benefit/risk ratio.”
In other words: for most menopausal women, in most cases, MHT is worth trying.
Buoyed by these eye-opening discoveries, I decide to make a leap into the unknown. I will give myself a six month experiential trial. Armed with knowledge, research papers and stroppy assertiveness, I set out to find help.
I try for an appointment in Wellington with a menopause specialist but there is a long waiting list due to the clinic only operating one day per week. There are a few private menopause specialists in Auckland and Christchurch but it will be an expensive consult if I need to travel to see them. I opt for a local approach under our public health system.
So I phone my local medical centre and ask for an appointment with a woman doctor who knows about menopause and prescribing MHT. I meet with a doctor who is very caring and helpful but doesn’t seem to know a lot about the treatment of menopause. I explain to her all my symptoms, omitting hot flushes which are not a big issue for me, and ask to be put on MHT.
Unfortunately not, she says. MHT is only prescribed for hot flushes and night sweats and she cannot prescribe it to me for other symptoms.
Here’s a list of symptoms that are very common for women to experience during perimenopause and menopause. Some of these symptoms can last more than a decade:
Hot flushes, night sweats, insomnia, brain fog, difficulty concentrating, decreasing short term memory, bladder and urinary issues, painful sex, depression, sadness, tension, anxiety, nervousness, mood swings, headaches, bloating, hand and feet swelling, heart palpitations, thinning hair, hair loss, brittle nails, allergies, tummy expansion, unpredictable periods (heavier, lighter, shorter, longer), vaginal dryness, joint pain, muscle aches, fatigue, poor sleep, loss of sexual desire, hair and skin changes, migraines, gum issues, loss of joy, dry and itchy skin, memory lapse, loss of confidence, vaginal atrophy.
Yes, there’s a real condition known as vaginal atrophy.
I change tack.
“I do get a few hot flushes,” I tell the doctor.
“How many?” she asks.
“Maybe 12 a day.”
“That’s a lot, “she says. “I can give you something for them.”
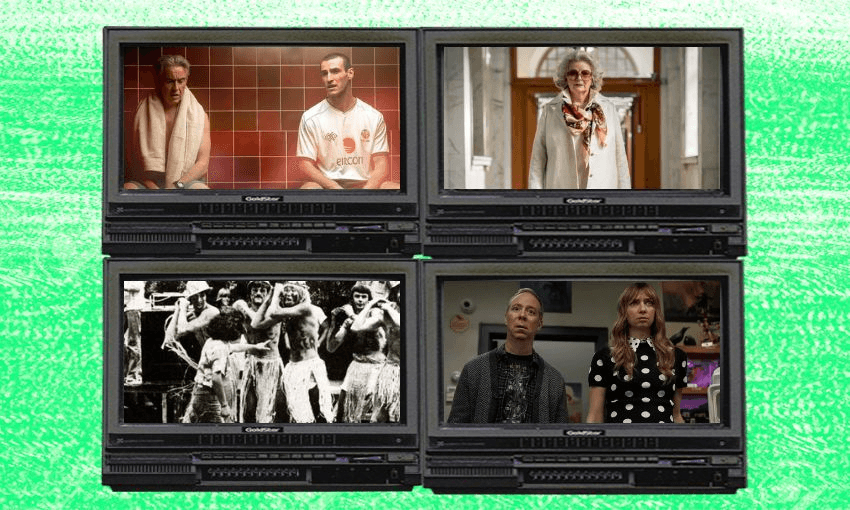
I have a shopping list ready:
“I would like Estrodot 25mcg Transdermal oestrogen patches and micronised progesterone Utrogestan, which isn’t subsidised but I’m happy to pay $32 each month for 24 tablets. And please throw in some Ovestin vaginal oestrogen cream as well.”
I will save my vagina from atrophy.
There is no evidence of increased risk of clot or stroke using transdermal oestrogen patches, at standard doses. There is a slight increased risk of breast cancer from taking MHT but it is less of an increased risk than from drinking two glasses of wine a day.
Even armed with this knowledge, I am aware I’m flying blind, self-medicating, reliant on information I find online. I enjoyed the drug experiments in my youth so I feel rebellious and excited to be trying out some legal but really difficult-to-obtain drugs in my sixth decade of life.
There is a noticeable difference within days. Over the next two months my joint pain disappears. My hips, knees and shoulder are pain free. I run down steps easily. I hike for six days through the Greenstone Valley in Fiordland and across the Routeburn Track.
I sleep through the night and the endless trips to the toilet day and night cease. My heart palpitations disappear. My brain reboots and joy returns in vivid technicolour. I have no desire for cake and my waist reappears. Oestrogen soaks into my cells and my world rotates again.
Six months ago I couldn’t write a shopping list. Today I am writing this article. I buy new dresses covered in bright spring flowers and throw away the black track pants.
Basking in a glowing light of renewed energy I approach my doctor for the last element in the MHT trifecta: testosterone.
Prior to menopause, women produce testosterone naturally in greater quantities than oestrogen. While the official expert position is that there is no evidence that it helps with the symptoms of menopause in older women, other research suggests testosterone cream in very small amounts can further increase energy, brain clarity and sexual desire.
I want a prescription.
The doctor looks like a startled rabbit in the headlights. “No, no, no I can’t do that.”
To be fair, she may have a point. While the research is promising, the lack of long term safety data on testosterone use in women means it’s not currently prescribed as a general tonic for those experiencing non-premature menopause. In New Zealand, testosterone’s only approved use among this group is for the treatment of hypoactive sexual desire disorder – low libido – which can be caused by the dramatically lower levels of circulating androgens as we age.
The side effects of excessive use of testosterone are serious and can be permanent. Experts say that women who use it should be monitored closely, including undergoing regular blood checks, to ensure levels remain within safe parameters.
While testosterone cream is unlicensed for menopausal women in New Zealand and the UK, it is available on prescription in Australia. Lawley Pharmaceuticals, an Australian company, makes testosterone cream for women called Androfeme. There is one pharmacy in Auckland that carries it.
My annual routine appointment at the public hospital is due so I target the gynaecologist. After our usual conversation about an ovarian cyst that she suggests could be removed and I say no, I tell her I would like to add testosterone to my MHT regime and need a script from her as it is an unlicensed medication. She has never prescribed testosterone to a woman patient before and knows little about it. She declines my request.
I tell her about Androfeme and point out that if it wasn’t for Covid I would be able to get some while visiting my son in Australia. I phone the Auckland pharmacy that prescribes it and the pharmacist agrees to email her the information.
I go home and wait. For three weeks.
A letter arrives in the mail. The gynaecologist hasn’t heard from the pharmacist so stands by her decision that testosterone is too risky, and she won’t prescribe it to me.
I phone the pharmacist myself and get the information emailed to me and forward it to the gynaecologist. I wait some more.
I email the gynaecologist again and coincidentally she is about to listen to a webinar produced by the Australian Menopause Society on the use of testosterone in women.
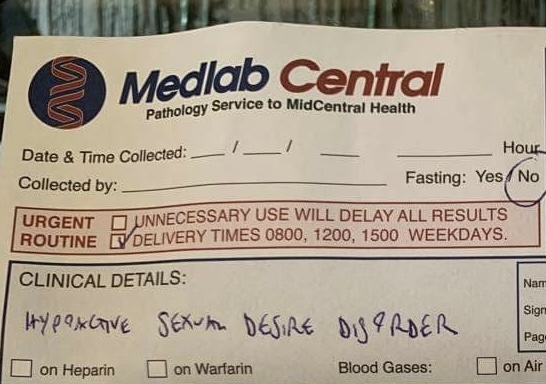
The next day I receive a questionnaire from her, which tells me I can only use testosterone if I have hypoactive sexual desire disorder. I answer YES to all the questions. She sends me a form to get my blood tested which has Hypoactive Sexual Desire Disorder written across the top. The lab technician smirks.
My prescription arrives in the post.
The pharmacist says she fills about 50 scripts for Androfeme per month. One tube lasts three months so that’s only 150 women rubbing a small dab of this particular brand of testosterone into their upper thigh per day in New Zealand. It costs $123 and arrives by courier.
On my first day of testosterone, I build a deck, fix the car, have a few beers with the boys and worry about my bald spot.
OK, the truth. After 12 weeks of use, I have so much more energy. I don’t come home at the end of the day and slump. I am active and motivated. Brain and body work in unison. I can exercise more intensely. I plant trees and make paths from heavy paving slabs. I cook meals from scratch. I have a renewed sense of purpose and vitality. My brain is back to how it used to be. Maybe better. My family notices I’ve returned from beyond.
My desire for sex has returned. Not in the way I imagined it would – it is not the desire I felt as a younger woman, nor is it a rampant testosterone-fuelled frenzy of desire. My body and brain now work in unison. I have energy to think about sex and to physiologically desire sex in a new way that fits with who I am now as an older menopausal woman.
While for me, testosterone was a miraculous addition to my MHT regime, I’m conscious of the risks. My gynaecologist is supervising the treatment and I’m undergoing regular blood checks to ensure I’m not over-dosing. I hope that in time my prescription can be transferred to my GP, to take some of the pressure off my overworked public health system gynaecologist.
At the community counselling centre where I’m a manager, we regularly receive referrals for counselling from local medical centres in our district. In 20 years, I have never seen menopause mentioned in a referral.
I have asked a few clients who fit the menopause demographic whether their GP has discussed menopause with them. They haven’t.
I ask if they think their symptoms might be related to menopause. Yes, they think they are related but they also seem as vague and uninformed about menopausal symptoms as I used to be.
I recently had a meeting with a new locum attached to one of the local medical centres to discuss our referral process. He told me that this particular medical centre never prescribed MHT. They don’t believe in it.
The natural decline in oestrogen, progesterone and testosterone may be a central cause of women’s depression, anxiety, despair and fatigue and one of the biggest reasons they are consulting medical and health practitioners. Many women are prescribed antidepressants but antidepressants will not help hormonal deficiency.
Before going through this transition myself, I had also misinterpreted some menopausal symptoms in clients as issues that I believed could be fixed through counselling. But we are not simply walking beacons of unresolved feelings and emotions. We live in hormone-fuelled bodies
The time frame of six months for my drug experiment has expired and I have no intention of giving up MHT.
I can comfortably live with the (slight) risks of using it. Life is risky at any age. Friends, colleagues and acquaintances around my age have started exiting this earthly realm from various cancers unrelated to MHT. Others have had aggressive treatments for cancers also unrelated to MHT and are thankfully still here.
In the history of humankind, the fact that women can live for up to 40 or even 50 years past menopause is so new that it wouldn’t even show up on a timeline. In 1929, the year my 92-year-old mother was born, life expectancy for women was 58 years.
In central Africa today, life expectancy for women is 56 years. I have been given a privileged gift of extra years and I am not going to spend it on the couch in a monochrome fog.
MHT may not suit every woman and many other women will sail naturally through the menopause transition.
However, information about menopause and available treatments needs to be accessible for all women so they can make their own choice and participate in a treatment plan that is right for them. All health professionals need to be educated, informed and comfortable having open conversations with women about menopause.
I am a stroppy, educated, professional woman and I still found it hard to access proven medication for my symptoms. But I got there in the end. Now I want all other menopausal women to have the same access to a therapy that has proven benefits that might just change their lives.